
Note from Shelley: Ron Rosedale‘s presentation was recorded live at the 2013 Annual International IPT (Insulin Potentiation Therapy) /IPTLE conference, held in Dallas. Ron’s title for the talk is, MTOR, INSULIN AND OTHER NUTRITIONAL ROOTS OF CANCER. Thanks to Debbie Curtis, Best Answer for Cancer and Ron Rosedale for permission to post the audio talk. (Transcript follows – including links to research studies)
LISTEN (1 hour) special thanks to Lynn Patrick for the music
Shoe  and the “Fit” of Life
and the “Fit” of Life

“One size shoe doesn’t fit all, but that shoe has to fit on a foot that attaches to a leg” – Ron Rosedale (image courtesy wikipedia)
RON ROSEDALE Thank you. I appreciate your being here, and I will try to make this interesting for you. There is a lot of information, and first, so that you don’t get too dizzy, I’m going to start out with an overview — a story. I know it’s been politically correct to say that one size shoe doesn’t fit all. But it’s really been my professional endeavor to find the mechanisms that do fit all, and I believe the similarities of life are far more significant than the differences because they remain similarities because life couldn’t get rid of them and still be compatible with life. So yes, one size shoe doesn’t fit all, but that shoe has to fit on a foot that attaches to a leg that has to run and hunt and gather and eat food to reproduce, and this is common to all life.
“Life, cell division and nutrition have been linked since the beginning of life.” Ron Rosedale (image courtesy Wiki)
There are certain fundamentals of life that we’ll be talking about. Life requires repair to stay alive, and to repair, one needs to divide cells. You need cell division. Cell division requires nutrients, so life, cell division and nutrition have been linked since the beginning of life. And to really find the answer to any disease, one needs to look at the roots of that disease, and look at why? Where did it arise from and then perhaps we might be able to arrive at a solution about how to treat that problem. So that’s what we’re going to do to begin with. We want to look at the history of life. Yep. Ten minutes — The history of life. In a nutshell.
It’s well established that life began in the oceans as single celled organisms. We know the ocean had plenty of glucose. Glucose was the primary fuel, deep down, in hydrothermal vents, there might have been some hydrogen sulfide, but after Life took hold, the oceans were swimming with single cell organisms feeding on glucose. And there was a lot more glucose than Life. So food restriction was not a problem and in fact, those who were to win at the evolutionary game were those that could eat the fastest. Could eat and process food and divide the most. It was a numbers game. Those who made the most numbers had the greatest chance at surviving. Basically, what we had was an ocean full of cancer cells. Later on, they evolved into colonies and then multicellular organisms.
Multicellular Organism courtesy dinopedia
Multicellular organisms are a little bit harder to divide. It takes more energy.
Life started eating other Life. So there was an arms race. There was Hunted and the Hunters. This required a better use of energy. There wasn’t just an endless supply of energy anymore. It was no longer necessarily those who could divide the fastest but those who could divide the best. And the signals for integrating nutrient availability and cell division, were laid down near the beginning of Life. In other words, if there’s a lot of nutrients available, let’s divide while the getting’s good. So there were signals that signaled cell division and that integrated nutritional availability with cell division.
As life started taking hold, plants formed in the ocean and put oxygen out into the atmosphere. Until this time, all energy use was anaerobic. This is an important aspect in Life’s history, because as the rules for cell division and integrating nutrients with cell division were being laid down and carried forward to this day, it was done in an anaerobic environment when Life was flourishing. It was long after Life began that oxygen started permeating the atmosphere from plants in the ocean and oxidative phosphorylation could be used. And instead of only being concerned with rate of cell division, Life began being concerned with the yield of cell division, as we are.
![]()
It’s not just a numbers game. We went from being concerned only with how long we divided, how rapidly we divided, to the quality of the division. We had to use fuel more frugally. There was less food, Life was more complex, and it behooved us not to waste energy so much.

Oxygen (image courtesy contrail science)
With this complexity of Life, it was a division of labor. As oxygen was put out in the atmosphere and multicellular organisms formed, some cells were on the inside and some were on the outside. By the way, when oxygen was put out, that was the first global polluting event, the worst polluting event in the history of mankind. Life couldn’t deal with that oxygen. It’s estimated that at least 90% of all life was wiped out, due to the oxidation. . . . until certain bacteria that we now call mitochondria were able to deal with that oxygen to actually use it to burn food, so they didn’t burn themselves. Those bacteria that could do that were then ingested by other bacteria and became our mitochondria.
There were two major events that took place as division of labor evolved. One was that cancer cells couldn’t be cancer cells anymore. They couldn’t just divide unrelentingly. They had to work for the common good. They had a specific job to do. And if they didn’t do that job, and they started behaving like cancer cells, they had to kill themselves. As far as becoming part and parcel of becoming part of multi-celled organism, they had to sign a contract that said they would do just that if they became more harmful than good. We call it apoptosis. That contract, by their neighbors, is revealed to these cells, as they start being cancer cells, and they’re supposed to kill themselves without harming everybody else. That’s apoptosis.

APOPTOSIS – a safe way for “broken” cells to shut down and recycle themselves
That was one major event that took place with division of labor. But an even more important division of labor that took place was between the genome and the soma. Previously bacteria, didn’t have a mortality. They would just divide into another bacteria and divide and divide. There was really no dead body, to say that this organism died.
But now, we basically separated out the genome and created a body around it to protect that genome. And the body said, “We’ll take the hits, and we’ll see to it that our genome stays intact long enough that we can pass that genome off to the next generation, like a runner in a relay race. We’ll take the baton, we’ll handle it well. We’ll protect it, and we’ll run until we can pass that baton off to the next runner. And that runner then has to take care of that baton and run around the track.

Passing the Baton – from waking times/wiki
But now, life had to make a decision. Because here we had a genome and a soma. The soma, after it hands off the baton, becomes expendable. Nature doesn’t need that soma anymore. In fact, it better get off the track, or it’ll get run over. That is the beginning of aging and mortality. That is why we die. That’s why we don’t stay alive forever, because the soma gets damaged so that we can preserve our progeny and hand it off. And we have to decide when to do that. When is it time to stop taking care of the body, allocate our precious resources toward reproducing, replicating the genome, whereas Nature no longer cares about the body anymore. There has to be a decision of energy allocation towards maintenance and repair of the body, versus reproduction. That’s dependent on nutrient availability. It takes a lot of energy to make babies. So there’s a connection now between nutrient availability, maintenance and repair versus reproduction. And there are important signals that have to integrate a whole bunch of cells that have a division of labor. And more importantly nutrient availability and whether to keep that soma, that body, that organism alive, basically so it can have a second wind, and continue running around the track holding that baton, or whether there’s enough nutrients available, and it’s a good time to hand that baton off and make a baby.

Mutiny on the Bounty from Wikicommons
All of our cells – Sometimes, the cells that make up our body, think, well you know our ancestors didn’t have to live and die just to take care of the genes. Why should we give our life to the genome? Why don’t we revert back to our old bacterial heritage, and just divide and divide and divide, so that we don’t have to die. Well, I know that we signed a contract that we would kill ourselves, but they say, Hey! Contracts are made to be broken. So they break that contact, and they start dividing and dividing and dividing, thinking they can be immortal, and when they do that, they sign their fate, because then they only have two choices. Either they win, meaning they kill their host, in which they die, or the host kills them and then they die. So when they cease to be a member of the republic, when they cease to be part of one with the Republic of Cells, when they cease do their job for the common good, they have now sealed their fate and they will die. instead of remaining virtually immortal and being passed on to the next generation.
So we must understand that cancer cells are healthy cells. They are not some weird, unhealthy, foreign cell. They are our bacterial heritage. They revert to their ancestry when they become cancer cells. It takes constant influx of signals to keep a cancer cell differentiated. Doing its job as part of the republic, being told constantly, don’t be a cancer cell. Don’t divide until I tell you to, until we need you to divide. Be a skin cell, be a liver cell, be a nerve cell. Do your job as part of the republic, and then we’ll all be better for it.

Clear Signals Matter
As such, when cancer cells revert, it’s because they’ve ceased to get those proper signals. And because of that, I consider cancer to be a default condition. It is what cells default to when they cease to get proper hormonal input. When they cease to get proper instructions on what to do, they become a cancer cell. That is what they default to. It’s not necessarily something they turn into.
They have it in them. That’s almost what they would prefer to do, given improper signals and the proper nutritional milieu that simulates what they were eating in the ocean. And what they were eating in the ancient oceans, so they could divide as bacteria, was glucose and they were using amino acids.

Cancer loves Protein
We know our ancient oceans were filled with glucose and amino acids. And that’s what our ancient cells ate, and that’s what our current cells, when they revert to cancer, eat. Sugars and amino acids is what they require for fuel and components to build themselves and reproduce. It hasn’t changed. So cancer likes glucose, lactic acid from glucose, and glutamine. Those are the three major nutrients that cancer feeds on today. Whether it be an aerobic or anaerobic environment, it reverts to its ancestral knowledge — what it knows, from its ancestors, which occurred in an anaerobic environment, so even if there is oxygen around, cancer cells try, and make lactic acid. That’s what aerobic glycolosis is. They will make glutamine, because glutamine then can be used to make component parts of that cell and can be used as fuel. It loves gluatimine, loves glucose, loves lactic acid.

Cancer Loves Sugar
We don’t need any of those. All of those are nonessential nutrients, so we don’t have to eat any of those.
So our job to stay healthy and reduce the risk of cancer, is to make cancer’s job as hard as possible. Don’t feed it. Make it hard for cancer to eat and divide.
It’ll do it anyway. It’ll make glutamine. It’ll make lactic acid. It’ll glucose out of anything els.e But we don’t ant to make it easy for it. The harder we can make it for the cancer cells, the longer it will take for cancer to divide, and it’ll give our immune system time to eat it. So we want to slow down cancer division, by not giving it want it wants, while we enhance our own immune system. That is the most powerful system we have to fight cancer, and it works remarkably well.
Now I’m going to show a bunch of slides and a bunch of studies, just to reiterate what I’ve said and bring us to the current state of where we’re at. But keep in mind our history, of what I just told you and you can understand why these studies are showing what they’re showing.
STUDIES AND REFERENCES
RON ROSEDALE: I’m hoping to really breeze through this so we have time for some questions at the end.
Understanding tumor cell metabolism: the secret to winning the war (burg) on cancer? Zachary T. Schafer (Seminars in Cell & Developmental Biology – Volume 23, Issue 4, June 2012, Pages 351)
QUOTE: “The plethora on information about cancer cell metabolism has been gleaned over the past few years, and has investigators to consider the possibility that cancer could be therapeutically eliminated through metabolic modulation. The idea is driving research on metabolic regulation of cancer cells in fascinating directions, and has even caught the attention of pharmaceutical companies.”
RON: This is one of the first studies that showed that dietary restrictions. .. . . My background is in the biology of aging, but the biology of cancer and aging are really married, because most animals die of cancer. When you slow down aging in a laboratory animal, almost universally, you’re slowing down the rate of cancer. Some strains die of autoimmune diseases. Mostly it’s cancer.
Calories Do Not Explain Lifespan Extension by DIetary Restriction in Drosophila, Mair W, Piper MD, Partridge L, PLoS Biol. 2005 July
RON: It was previously thought that dietary restriction or calorie restriction, it’s being shown that it’s not just calorie restriction. Calorie restriction extends lifespan in all organisms. But (quoting from the study)
QUOTE: “The reduction of either dietary yeast or sugar can reduce mortality and extend lifespan by an amount unrelated to the calorie content in the food, with yeast having a much greater effect per calorie than sugar. (Yeast is mostly made of protein.) Calorie intake is then not the key factor in the reduction of mortality rate.”
Prospective Study of Hyperglycemia Risk and Cancer, P. Stattin, Diabetes Care 2007
QUOTE: “The association of hyperglycemia with total cancer risk in women and in women and men combined for several cancer sites, independently of obesity, provides further evidence for an association between abnormal glucose metabolism and cancer.”
Lactate, is like ‘candy for cancer cells’: Cancer cells accelerate aging and inflammation in the body to drive tumor growth.
QUOTE “Cancer cells initiate a “lactate shuttle” to move lactate — the “food” — from the connective tissue to the cancer cells. There’s a transporter that is “spilling” lactate from the connective tissue and a transporter that then “gobbles” it up in the cancer cells. . . . The researchers see that lactate is the candy for cancer cells, and cancer cells are addicted to this candy.”
BASED ON THIS STUDY: Michael P. Lisanti, M.D., Ph.D., Professor and Chair of Stem Cell Biology & Regenerative Medicine at Jefferson Medical College of Thomas Jefferson University and a member of the Kimmel Cancer Center. 2011, Cell Cycle
Metabolic reprogramming in cancer: unraveling the role of glutamine in tumorigenesis. Semin Cell Dev Biol. 2012 Jun;23(4):362-9.
QUOTE: Increased glutaminolysis is now recognized as a key feature of the metabolic profile of cancer cells, along with increased aerobic glycolysis (the Warburg effect). In this review, we discuss the roles of glutamine in contributing to the core metabolism of proliferating cells by supporting energy production and biosynthesis. . . . cells coordinate glucose and glutamine as nutrient sources.
RON: Cancer cells initiate a lactate shuttle. They make their own lactate. They want lactate. To move lactate from food, there’s a transporter that’s spilling lactate from the connective tissue, and a transporter that then gobbles it up in the cancer cells. The researchers see that lactate is the candy for cancer cells, and cancer cells are addicted to this candy. It is what they want. We don’t want to give it to them.
Is there a role for carbohydrate restriction in the treatment of cancer? Rainer J Klement, Nutr Metab (Lond). 2011; 8: 75.
QUOTE: “Over the last years, evidence has accumulated suggesting that by systematically reducing the amount of dietary carbohydrates (CHOs) one could suppress, or at least delay, the emergence of cancer, and that proliferation of already existing tumor cells could be slowed down. . . . CHOs or glucose, to which more complex carbohydrates are ultimately digested, can have direct and indirect effects on tumor cell proliferation: first, contrary to normal cells, most malignant cells depend on steady glucose availability in the blood for their energy and biomass generating demands and are not able to metabolize significant amounts of fatty acids or ketone bodies due to mitochondrial dysfunction. Second, high insulin and insulin-like growth factor (IGF)-1 levels resulting from chronic ingestion of CHO-rich Western diet meals, can directly promote tumor cell proliferation via the insulin/IGF1 signaling pathway. Third, ketone bodies that are elevated when insulin and blood glucose levels are low, have been found to negatively affect proliferation of different malignant cells
RON: There are all sorts of ways that eating a high carbohydrate is really bad for us, great for cancer.
STUDY: Insulin analogues and cancer risk: cause for concern or cause célèbre?, M Pollak, Int J Clin Pract. 2010 Apr;64(5):628-36
RON: Twenty years ago, I wrote an article that said your insulin may be killing you. This was 20 years ago. Boy did I get hate mail from around the world from physicians. It was unknown at that time. But this (shown above) is a more recent article.
QUOTE: “insulin and insulin analogues can function as growth factors and therefore have theoretical potential to promote tumor proliferation. Analogues causing inappropriate prolonged stimulation of the insulin receptor, or excess stimulation of the IGF-1 receptor, are the most likely to show mitogenic properties in laboratory studies. Some recent epidemiological studies appear to be consistent with these experimental findings. . . . it is biologically plausible that hormonal factors that influence neoplasia could begin to manifest their effects in surprisingly short timescales (within 2 years) and hence these epidemiological studies justify further research.”
RON: When they talk about analogs, they’re talking about insulin injections. This is what we give to diabetics, who are now having very high rates of cancer. They grouped five epidemiological studies that showed there was a huge increase in cancer among those people who were taking insulin. Now they’re saying, maybe we should ignore that because it happened within two years. That’s fast when you’re talking about cancer. It justifies further research.
PROTEIN & CANCER
RON: You’re going to hear me talking a lot about protein. For many many years, I talked about the detriments of glucose and insulin. I talked about leptin. When I first got into it, there was really just a handful of people espousing a low carb diet. Myself being one, there was Atkins, there were Mary and Dan Eades and Barry Sears. And that was it. I was going around the world. Out of those, I was the only one talking specifically about a high fat diet. The others were espousing a high protein diet. And all along, I’ve shown that high protein is not good. You’re going to hear me talking a lot more about that now. It’s finally getting some traction because of an enzyme called MTOR that we’re going to talk a lot about.
Effects of dietary protein restriction on glucose and insulin metabolism in normal and diabetic humans, Larivière F. Metabolism. 1994
QUOTE: “After adaptation to the protein-restricted diet, diabetic subjects experienced a 30% decrease in … blood glucose … this occurred despite a concurrent 25% decrease in both basal and bolus insulin dosages
RON: In other words, they’re getting more insulin sensitive.
QUOTE: “We conclude that severe protein restriction decreases insulin requirements in type I diabetes and fasting hepatic glucose output and basal insulin levels in normal subjects. This effect appears to be mediated in part by decreased hepatic gluconeogenesis, but a contributory influence of increased insulin sensitivity is not ruled out.”
The role of insulin and IGF-1 signaling in longevity, Katic M, Cell Mol Life Sci. 2005 Feb
RON: Growth hormone. People take growth hormone to reduce aging. That’s nuts.
QUOTE: “Insulin and insulin-like growth factors represent a family of hormone growth factors that regulate metabolism, growth, cell differentiation and survival in most tissues in mammals. . . . Insulin and IgF initiate their action via a highly homologous signaling pathway.”
RON: They’re cousins. IgF and insulin arose from a common ancestor. In worms, it’s insulin/IgF. They do the same thing. Then there was a division of labor and IgF was assigned more of the anabolic functions of insulin, and insulin more of the metabolic functions. Although they cross-react with one another other, and they can each bind to the other’s receptor. So insulin is a growth factor just like IgF, and IgF can be be a metabolic factor and lower glucose.
QUOTE (from The role of insulin and IGF-1): The most striking and most consistent model of extended lifespan and one which dramatically demonstrates the role of metabolism is calorie restriction. Indeed, calorie restriction retards aging and extends median lifespan in yeast, worms, fish, flies rats monkeys, and recent data suggests even humans. Some of the common and consistent findings in rodents and non human primates include lower fat mass, particularly visceral fat, lower circulating insulin and IgF concentrations.
RON: In other words when you calorie restrict and you extend lifespan, you almost universally lower insulin and and growth hormone. Why would you want to take it?
QUOTE: You have increased insulin sensitivity, lower body temperature
RON: . . . and I should also add, as a result, lower free T3. Not high. I know there’s a big thing going on in the paleo community that I’m fighting.
Lower fat free mass, lower sedentary energy expenditures. Decreased levels of thyroid hormone and decreased oxidative stress.
QUOTE (The role of insulin and IGF-1 ) One of the striking physiological characteristics recently identified in centenarians is a greatly increased insulin sensitivity compared with younger subjects. Centenarians living in Southern Italy showed that this group have a preserved glucose tolerance and insulin action and lower plasma IGF-1 levels compared with aged subjects.
RON: So not just in calorie restricted animals. In centenarians you have virtually a totally parallel finding to those you find in calorie restricted animals. With lower temperature. Lower thyroid. I should say also, higher cortisol levels, not lower. That’s also what you find in calorie restricted animals. You have to understand, cortisol is an anti-inflammatory. Everybody equates high cortisol to horrible. It’s not. Just how it’s being used is inappropriately.
QUOTE (The role of insulin and IGF-1 ) In conclusion, Strong similarities exist between insulin and IgF signaling systems, in yeast, worms, flies . . . These may be linked to oxidative stress resistance, metabolic regulation, food utilization and lifespan in each of these organisms. They suggest that insulin IGF system arose early in evolution and is a central component of an anti-aging system that is conserved from yeast through humans.
RON: It is a commonality. It is is not different shoes for different people. I don’t care if you’re a yeast, if you’re a worm, if you’re a mouse, if you’re black, Asian Caucasian. If you eat a non-fiber carbohydrate, it will raise your glucose levels. It will raise insulin. It will raise IgF. If you eat protein, it will raise MTOR, it will raise leptin. It will do this in every animal. And these are the commonalities we have to look at. In some people it will raise it more than other people. You can fine tune it later. But fist, let’s look at the foundation of life. Because that’s what we have to manipulate if we want to preserve it.
The role of the insulin-like growth factor-I receptor in malignancy: an update, Seccareccia E, Growth Horm IGF Res. 2012
QUOTE: It is now well documented that the role of the IGF system extends beyond the initial steps of malignant transformation, and includes the later stages of tumor progression. And the multiple steps required for metastasis. Indeed the IGF axis has been validated as a target for cancer therapy.”
Obesity Linked to Aggressive Prostate cancer, Science Daily, 2003
QUOTE: “. . . suggest that proteins and hormones stored in body fat – such as leptin and insulin-like growth factor-1 – may promote prostate tumor growth in obese men. Also, obese men typically have lower testosterone levels and higher estrogen levels, which may encourage the growth of cancer.”
Caloric restriction, slowing aging, and extending life. Masoro EJ, Science, 2003
QUOTE: “Mice with pituitary glands devoid of growth hormone producing cells exhibit a mildly extended lifespan, as do genetically engineered mice with a targeted disruption in the growth hormone receptor, which results in low concentrations of IgF.”
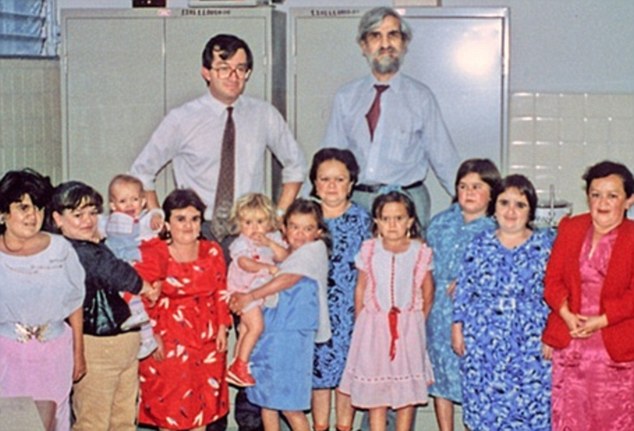
Ecuadorian Dwarfs have less cancer & diabetes – photo from Daily Mail/Wiki Commons
Dwarfism Gene May Offer Protection From Cancer, Diabetes
RON: This is a family in Ecuador. that has something called Laron Syndrome. Scientists are studying these people because it’s a model for low growth hormone, and they find – Valter Longo is the one that’s leading this study. He’s a well known aging researcher.
QUOTE: Longo has long been interested in the genetics of aging. He and others have found evidence in yeast, worms and mice that restricting growth hormones could make those creatures live longer.. . . . Guevara-Aguirre had diagnosed family members with Laron Syndrome, a rare syndrome caused by a gene mutation in growth hormone. Over the course of his years with the family members, he noticed that people with Laron syndrome almost completely avoided cancer and diabetes. An observation that squared with research Longo and others had done in yeast and animals. Longo hypothesized that it could be because cells must invest energy in either trying to grow and produce, or in protection.
RON: In other words, maintenance and repair or reproduction. Energy, as life progressed, was just not available everywhere, so you had to make a decision. Keep the soma alive or reproduce.
SCIENCE DAILY: ’Un-growth hormone’ increases longevity, researchers find, December 23, 2010, Saint Louis University
QUOTE: A compound which acts in the opposite way as growth hormone can reverse some of the signs of aging, a research team has shown. The finding may be counter-intuitive to some older adults who take growth hormone, thinking it will help revitalize them. . . . Overall, the researchers found that MZ-5-156 had positive effects on oxidative stress in the brain, improving cognition, telomerase activity (the actions of an enzyme which protects DNA material) and life span, while decreasing tumor activity.
RON: He says that most life, and people, are stuck in a pro-growth mode. This study confirms our strong position that studying the basis of aging can give a much better payoff than studying each disease in nature individually. Dwarf models live longer. Ponies live longer than horses. Small dogs live longer than large dogs. It’s a very fascinating field in aging. So, they make a drug to reduce growth hormone — MZ-5-156, had positive effects on oxidative stress in the brain, improving cognition, telomerase activity and lifespan while decreasing tumor activity.
MZ-5-156, like many growth hormone receptor antagonists, inhibited several human cancers including prostate, breast, brain and lung cancer.
RON: They’re making drugs to lower growth hormone, and people are taking growth hormone (thinking) they’ll live longer.
Long-term effects of calorie or protein restriction on serum IGF-1 and IGFBP-3 concentration in humans, Luigi Fontana, Aging Cell. 2008
QUOTE: Protein increases the levels of insulin, IgF and Leptin. Our data provide evidence that protein intake is a key determinant of circulating IgF 1 levels in humans and suggests that reducing protein intake may become an important component of anti-cancer and anti-aging dietary interventions.
RON: So you don’t need a drug. Just don’t take so much protein, and you’ll lower IgF better than you will with a drug.
Central Nervous System Control of Food Intake and Body Weight, G. J. Morton, Nature 2006,
QUOTE: “Genetic and pharmacological studies suggest a more critical role in leptin than insulin in mammalian energy homeostasis.”
RON: Many people know nothing about leptin, still. Hardly ever being routinely tested. And if I had to pick 1, and I did recently – I got interviewed — somebody’s writing a book about laboratory testing, Asked me to pick one test that I would pick as being the most important and I picked leptin. It is leptin. It regulates everything else that you test.
The role of leptin in leptin resistance and obesity, Zhang Y, Physiol Behav. 2006
QUOTE: Results from multiple studies demonstrate that (1) chronically elevated central leptin decreases hypothalamic leptin receptor expression and protein levels and impairs leptin signaling; (2) leptin resistance and obesity are associated with reduced leptin receptors and diminished maximal leptin signaling capacity; and (3) leptin resistance confers increased susceptibility to diet-induced obesity. In essence, the augmented leptin accompanying obesity contributes to leptin resistance, and this leptin resistance promotes further obesity, leading to a vicious cycle of escalating metabolic devastation.
RON: This is really important. People who do know about leptin think that it’s determined by how much fat you have. That is not true. It’s determined more by what you eat. Your leptin levels fluctuate, widely throughout the day, depending on what you eat, except most people eat the same thing. Most people eat a high carbohydrate diet, high protein – your leptin levels will stay high. If you change your diet today, your leptin can be half of what it is today, tomorrow. And when you lower leptin, you improve leptin sensitivity. And when you improve leptin sensitivity, your body then can speak to your brain and tell it how much fat it has. It can say, you’ve got too much fat. You’d better get rid of it, or you’re not going to be healthy and you’re going to get eaten by a lion, because if it’s chasing a group of people, it’s going to catch you.
Leptin regulates pro-inflammatory immune responses.
QUOTE: These results identify an important and novel function for leptin: up-regulation of inflammatory immune responses, which may provide a common pathogenetic mechanism that contributes to several of the major complications of obesity.
RON: . . . including cancer.
Obesity may accelerate the ageing process
RON: Leptin itself is a pro-inflammatory cytokine that is also a key component in fat that initiates the manufacture of many other inflammatory chemicals. Interleukin. TNF alpha. It’s critical for health, and hardly anybody knows anything about it, and doesn’t realize that it’s highly modulated by diet.
QUOTE (From Obesity May Accelerate): Intriguingly, the link between high leptin concentrations and telomere shortening was even stronger than the link with obesity.
RON: Now, I wrote an article (for Mark’s Daily Apple), so that if people want more information about telomeres . . .
RON: Telomere testing right now is mostly testing for immune cell turnover. Basically telomeres and white blood cells. So all it’s really telling you is how rapidly your white blood cells are turning over, and if you’ve got a lot of inflammation. So it’s basically an expensive marker for inflammation. To me, it’s not a great test. There’s a lot more that has to do with telomeres. But leptin will tell you the state of your inflammation, and you can predict the attrition of telomeres by leptin concentrations. That’s all you need.
QUOTE: Thus, in normal men, the fall in leptin with fasting may be both necessary and sufficient for the physiologic adaptations of these axes.
RON: In other words, in calorie restriction and starvation, there is a shift in metabolism toward longevity. Leptin is necessary for this.
PPARα activators may be good candidates as antiaging agents
RON: I put this in for a reason.
QUOTE: Cellular damage in aging is at least in part the result of fatty acid excess secondary to leptin resistance. So we come to the conclusion that youth is a leptin sensitive state, and a resistance to leptin occurs with aging. . . . Increased plasma leptin levels with aging suggest resistance to leptin action, and may explain why elderly subjects have abdominal obesity and insulin resistance. Leptin’s failure may be seen with the metabolic decline of aging.
RON: But look at the title again: PPAR alpha activators may be good candidates as anti-aging agents. I talked about this a long time ago, because PPAR alpha is virtually the opposite of PPAR gamma. PPAR alpha initiates fatty acid beta oxidation. PPAR gamma initiates lipogenesis. So all the drugs that were being used for so long for diabetes were PPAR gamma agonists, and then they wondered why they were killing people. Because they were pro-aging. It’s good to know a little about aging. It gives you the bottom line.
New drug to tackle fat problems
QUOTE: Leptin, the obesity hormone, is produced by fat and excess leptin predisposes overweight people to conditions such as multiple sclerosis, cancer and heart disease whilst a deficiency in leptin, as occurs in malnutrition, results in infertility and immunodeficiency.
RON: Again. Looking for drugs. Do it with diet. You can do it today. Far better.
Regulation of leptin secretion from white adipocytes by insulin, glycolytic substrates, and amino acids
QUOTE: amino acid precursors of tricarboxylic acid cycle intermediates potently stimulate basal leptin secretion per se, with insulin having an additive effect
RON: Again, it is amino acids that can stimulate leptin in the presence of glucose or not. Because glutamate will stimulate it without glucose or insulin. High protein can raise blood glucose. Produce insulin. It increases glycation. Oxidative damage. It increases IgF. Protein increases leptin. Triggers Hexosamine, which causes insulin resistance. Life is a constant battle between damage and repair, and excess protein increases the damage and reduces our ability to repair it. High protein accelerates aging. Reducing protein extends life. Why? mTOR. Huge. So, (showing a very complex chart) I want you to memorize this. What this is is a picture of two robotic spiders mating. (switching to another chart.) But here we have something we can sink our teeth into, maybe. There are just a few things here that I want you to notice. mTOR is kind of two fractions. It’s a complex. Here’s mTOR 1 and here’s mTOR complex 2. And I want you to notice that mTOR-1 inhibits autophagy. Autophagy is necessary for long life. Cancer cells don’t like it. As you raise mTOR you inhibit autophagy — likewise, as you lower mTOR you increase autophagy, and it extends life. They have found now that the reason calorie restriction extends lifespan is because of the inhibition of mTOR. It’s critical. I also want you to notice something else. Amino Acids. Amino acids stimulate mTOR directly. In other words, they act as hormones. Critical that people know this. Doesn’t do it through insulin.
RON: Here are growth factors. Insulin, IgF. They stimulate actually mTOR-2. mTOR-2 is involved in apoptosis and other things, too. So both of them are very involved in aging and cancer. But stimulated by amino acids, growth factors, insulin and igf, which are raised by what? Glucose and protein. Right? Then you have glucose here increasing mTOR-2, in a roundabout way.
RON: So this is what I want you to know. Glucose, insulin and Ifg, which is mediated by glucose and protein . . . Amino acids, protein, and here, went, (shows another part of the chart) and the only reason I bring this up because the people who discovered this and named it, “Frizzled 7 and Dishevelled,” obviously didn’t get enough sleep. But these are some of the things it regulates. Gene expression, mitochondrial proliferation. Metabolism and stress response, apoptosis and lipid synthesis, which is necessary for cancer cells.
mTOR: from growth signal integration to cancer, diabetes and ageing
QUOTE: In all eukaryotes, the target of rapamycin (TOR) signaling pathway couples energy and nutrient abundance to the execution of cell growth and division, owing to the ability of TOR protein kinase to simultaneously sense energy, nutrients and stress and, in metazoans, growth factors. Mammalian TOR complex 1 (mTORC1) and mTORC2 exert their actions by regulating other important kinases, such as S6 kinase (S6K) and Akt. In the past few years, a significant advance in our understanding of the regulation and functions of mTOR has revealed the crucial involvement of this signaling pathway in the onset and progression of diabetes, cancer and ageing.
In all eukaryotes, us, the target of rapamycin — mTOR, is a signaling pathway that couples energy and nutrient abundance to the execution of cell growth and cell division owing to the ability of mTOR protein kinase to simultaneously sense energy, nutrients and stress in metazoans. In the past few years, a significant advance in our understanding of the regulation and the functions of mTOR has revealed the crucial involvement of this signaling pathway in the onset and progression of diabetes, cancer and aging. Target of rapamycin was originally discovered in yeast but is conserved in all eukaryotes including plants, worms, flies and mammals. In other words, all of us. One shoe does fit all.
Mammalian mTOR controls growth and response to nutrients, amino acids, growth factor, insulin, IgF. As a central control of growth and metabolism, mTOR plays a key role in development and aging and is implicated in many diseases including cancer, cardiovascular disease, inflammatory disease, metabolic disorders. Indeed, it has been calculated that mTOR is up-regulated in 70% of all tumors. You can’t really treat cancer without knowing about mTOR, as far as I’m concerned.
The PI3K/AKT/MTOR pathway is important in many types of cancer. The measurement of active AKT and other pathway components in human tumors has revealed that pathway activation is one of the most common molecular alterations in human cancer.
Discordant regulation of the p53 and mTOR pathways. What it is showing is a connection between p53, the apoptosis gene, and mTOR. Amino acid sensitive mTOR. In other words, this is just showing that mTOR is an ancient effector of cell growth . It integrates signals from growth factors and nutrients. Indeed, mTOR was determined by amino acid availability. That’s what determines mTOR.
More – this shows again – Amino Acids. Amino acid signaling and integration of metabolism, Nutrient sensing mTOR pathways regulate leptin production. mTOR is activated by 3 fatty acids. We propose that mTOR may may ben an appropriate nutrient sensor for leptin expression in adipose tissue. And yet leptin induced mTOR activation may have implications for obesity. They speak to each other. Leptin and mTOR are the two most important metabolic pathways in the body that will determine whether you are healthy or not. And most people know nothing about either of them.
We found a major pathway by which amino acids control mTOR signaling which is distinctive from that of insulin. In other words, the amino acids themselves act directly as hormones.
Rapamycin is an inhibitor of mammalian target rapamycin. It increases cellular stress response, characterized by rapid and sustained activation of apoptosis kinase 1.
It signals the apoptosis and selective apoptosis of cells lacking functional p53. In other words, it doesn’t have to work through p53. Most cancer cells have mutated p53. They bypass the apoptosis. Well, you can still kill them by regulating mTOR because it doesn’t need p53 to activate apoptosis.
So they make a drug now, that targets mTOR.
mTOR acts as important regulator of cell division, blood vessel growth, cell metabolism, resistance to hormonal therapy in breast cancer, it has been associated with over activation of the mTOR pathway –
The best drug to slow aging and chronic diseases associated with aging is already available – avoid high protein. Critical.
We find that in treating mammalian cells, we find that rapamycin treatment results in a gene expression profile . . .
mTOR stands for the mammalian target of rapamycin. Rapamycin they found and then the learned how it worked – It inhibited mTOR, and that’s how it worked to alleviate cancer. So they knew this. It was an old fold remedy. Drug companies then isolated what it was that rapamycin was doing to inhibit cancer – and they found a whole knew pathway that they never knew existed in 1994 or so . . . That was the target of rapamycin, they called it. Rapamycin was known before mTOR, as an inhibitor of mTOR that could treat cancer.
Rapomycin treatment results in a gene expression profile that resembles one seen with amino acid limitations. So if you restrict amino acids, you are taking one of the most powerful anticancer drugs known to man.
Lucine deprivation proves deadly to malignant melanoma cells.
An anti-Atkins, low protein diet extends lifespan. And it provides significant advance in the understanding of the role of TOR.
A recent study appearing in Nature showed that feeding rapamycin to mice limited Tor and extended their lifespan.
So what’s high?
For me, above 1 gram per kilogram per day of your estimated lean mass is what a person should be on, and no more, and if you’re treating cancer, I’d go lower. I’d go to .7 grams per gram of lean mass per day. And even lower if it’s an aggressive cancer. You could easily go to .6 grams per kilo of lean mass per day, in divided doses. You’re getting enough to keep your SELF going, and you’re not overfeeding the mouth, and you’re not overstimulating mTOR. In other words, you do not want a low carbohydrate, high protein diet.
You want low carbohydrate. You don’t want to be feeding the cancer sugar. You don’t want to be feeding it lactate. You don’t want to be up regulating insulin/igF by a high carbohydrate diet. So yes, you do want a very low carbohydrate diet. But most people who go to a low carbohydrate diet eat way too much protein.
Therefore, they’re not seeing the potential great benefits that you could see with a very low carbohydrate
What you want to eat is fat.
What I wanted to point out, actually, in that fancy diagram we had up there, and all the things that were stimulating mTOR – IgF, glucose, amino acids. What is glaringly missing from everything I’ve talked about so far today?
Fat. It’s a free ride. Why is that? Go back to what I said to begin with. All of these pathways, these aging pathways, these pathways that control cell division and therefor cancer, developed in an anaerobic ocean. Fat could not have been used as fuel at that time because you cannot burn fat without oxygen. So all of these rules that were laid down to regulate lifespan and cell division were done using glucose and amino acids as fuel and components of the manufacture of cells. The use of fat as a fuel didn’t happen until almost three billion years later.
So you can eat fat. It doesn’t raise insulin. It doesn’t raise IgF. It doesn’t raise mTOR. And oddly enough, it doesn’t raise leptin. Leptin is regulated by glucose and amino acids. So if you eat a really high fat diet and keep your protein moderately low – we have to have some. Carbohydrates, you don’t have to have any. It’s a non essential nutrient. You can go as low as you want.
Carbohydrates, it’s just fiber or not fiber. Fiber is great, and not that it’s essential. It’s just that it doesn’t turn into glucose. It might scrub your intestines, and soluble fiber can be turned into short chain fatty acids – good for your colon. That’s great. But any carbohydrate that is not a fiber will turn into sugar that will cause harm. It’ll glycate, it’ll raise insulin, it’ll cause cancer. You don’t want it. The lower the better. You don’t have to worry about getting too low, in other words.
We have to have some protein. The key is how much. Too much is terrible. So there can be some fudge on how much, depending on circumstances. If you work out. If you’re pregnant, if you’re growing. You need a little bit more. But if you’re trying to treat cancer and you’re an adult, you want to go on the low end of the scale, which I would go to .6 grams per kilo of lean mass, per day. If you’re healthy, maybe 1 gram per kilo of lean mass per day, in divided doses.
The protein content of breast milk is only about 1 gram per 100 milliliters, and the daily protein intake is approximately 1 gram per kilo per day. This is in an infant. It is doubtful that you will have require that much.
You’re growing more than you will ever grow.
You cannot sit on a couch, eat a bunch of protein and expect your muscles to grow. It doesn’t work that way. Athletes constantly say, eat a high protein diet because you will build more muscle. No you won’t. You need to modulate the signals to build muscles.
You don’t take calcium to build bones. Calcium does not build bones. Signals build bones. We know lowering leptin will build bones. It’s modulated. If you have signals to build bone, and that means, the protein in the bone, which is what confers strength. Calcium has nothing to do with that strength, and in fact, calcium will interfere with those signals.
What’s left to eat – fat. A moderately high fat diet is associated with lower than expected circulating leptin concentrations. If you lower leptin, you’ll improve leptin sensitivity.
Can a high fat diet beat cancer? The answer is – Yes.
Clinical diet, a study I published with Eric Westman at Duke, showed that . . . If you follow this type of diet, you get the same laboratory changes you see in calorie restricted animals without calorie restricting. You reduce glucose, you reduce insulin, you reduce free T3, you reduce body temperature, and there’s a 50% reductions in insulins, leptin and triglycerides and free T3.
Same thing that you can do with calorie restriction but you don’t have to calorie restrict. It’s a lot easier. In other words, fat is a free ride. You can eat fat and you can have the same benefits as calorie restricting. It’s not calorie restricting. I showed that earlier.
Your health and lifespan will mostly be determined by the proportion of fat versus sugar you burn over a lifetime. I’ve said that for 20 years. I’ve not found anything to contradict it. All the evidence that has occurred in the last 20 years has supported that one statement. Everything there is to know about health, and aging, can be summarized right there. Your health and lifespan will be determined by the proportion of fat versus sugar that you burn over a lifetime.
If you burn sugar as your primary fuel, which the vast majority of people in the world are doing, you’re not going to be healthy. You’ll have a high risk for cancer. If you use fat as your primary fuel, you’ll be much healthier.
And whether you burn fat or sugar, is determined by hormones. It’s going to be determined by insulin and leptin and mTOR, and those in turn, and those, in turn, are affected by what you eat. So what you eat are basically the most important hormones that you are going to be exposed to. Because they then, affect the “Generals” of metabolism that sends signals to every other cell and every other pathway and every other hormone to do their bidding.
In other words, what this will tell you is that diabetes is not a disease of blood glucose. Glucose is just listening to orders.
Don’t take drugs to lower glucose. Do something that affects the instructions from high up. From leptin and insulin and mTOR. And they’re affected by what you eat. That will be determined by the communication of hormones, insulin, IgF and leptin. Life is not in the parts. We are all made of the same stuff. Don’t just treat the parts. You won’t get anywhere. It is what you, or more accurately, your hormones, do with the parts, that determines your health and life. If I were to die right now, my parts would remain the same. I’d have the same calcium. I’d have the same glucose. I’d have the same cholesterol. That’s not what’s killing me. If I were to die right now, what’s killing me is the harmonious integration of those parts, which has been lost. I’m no longer a Republic of Cells. I’m a bunch of disparate parts, that aren’t getting instructions, and that’s what you see with cancer. Each cell going for itself. To be healthy, you have to have 15 trillion cells and 90 trillion bacteria working collectively and harmoniously for the common good. And the way you do that is by eating properly.
Thank you. Now I will take questions.
QUESTION: I find it interesting that Max Gerson would recommend in his day, a diet that was very low in starchy carbohydrates, and very low in animal source proteins, and he had great results. The same thing for Johanna Budwig. Also from Germany.
RON
Yes, she recommended flax seed . .
QUESTION: Flax seed and flax seed oil, and a bit of fermented organic. Great talk. Appreciate it tremendously. The only thing to add is fats are good in cancer, but the wrong fats are really bad in cancer The really bad fats are the oxidized fats, the trans fats, the peanut oil, the canola oil, and the Omega 3/Omega 6 imbalances.
RON
That’s a great comment – I just didn’t have time to talk about it. To me, just really quickly, all of nutrition is really simple. Carbohydrates – fiber or not fiber. The less non-fiber carbohydrates the better. Protein, I don’t care where you get it, for the most part. It’s a matter of how much. That’s critical. Fats to me is where 95% of nutrition lies. The rest to me is really cut and dried. I didn’t have time to talk about what are the good fats and what are the bad fats. Omega 6s are terrible, because they do oxidize, and we have a huge Omega 6 to Omega 3 ratio imbalance. There’s no question about that. Heart disease is caused by the oxidation of cholesterol. It’s not caused by cholesterol itself. Cholesterol is your friend. It is there to keep you alive. So I’m really glad that Dr. C – thanks a lot for bringing that up. Yes there’s a huge difference between kinds of fats.
QUESTION: Great presentation. Thank you. You didn’t mention the difference between animal protein and plant proteins. In the China Study by T Collin Campbell, there was a great distinction – the animal proteins being carcinogenic, and plant proteins being not, or somewhat protective. Would you care to comment?
RON:
First of all, the China Study has so many flaws in it that it’s a worthless study. But most of the time, when they’re eating plant proteins, a lot of them are less digestible. And so they’re actually intaking a lot less protein. So it’s a lower protein diet, which is good That being said, the most important aspect is how much you’re eating. Is there a difference between kinds of protein. Yes there is.There are certain amino acids that stimulate mTOR more than others. Lucine is the major amino acid that stimulates mTOR. And you’ll find more lucine in animal protein. There are less mTOR stimulating acids in plant proteins than there are in animal proteins. But the volume of protein you eat is going to outweigh the kind of protein.
QUESTION: One more thing about the protein. Tyrosine is a substance that’s known to increase cancer and it’s much higher in animal proteins than in plant proteins.
RON
Yes. Thanks
QUESTION: Through nutrigenomics testing I can see what kinds of fats different gene types require and what percentage. How does that figure in to what you’re talking about?
RON
I think that nutrigenomics and metabolomics, basically we’re talking about differences among people. I don’t want to say differences between people are irrelevant. They’re not. They can influence digestion. They can influence gut flora, for instance. We’re pretty complex. But I think what we have to get down first is the foundations. That, for instance, we know that you or me or anybody who eats a piece of bread is going to raise their blood glucose. Guaranteed. It can be a worm, it can be a fly. It will cause harm. The difference between you and me is how much harm is going to be caused? That harm is going to be determined by how rapidly glucose is going to rise in your or me. It’s going to be determined by how much that glucose affects insulin and how rapidly it rises and how much it rises. Two people can be exposed to the same amount of glucose, and one person it might raise their insulin to 30 and in another it might raise to almost 300 – I found in a child who was obese. He was insulin sensitive, but he had a very hyper insulin response to eating a certain amount of carbohydrate. The type of gut flora you have in you is going to have an affect on your glucose and insulin. We definitely have differences, but what we want to find are commonalities. And we know that protein is the major component that will raise mTOR, and if you raise mTOR it will do all those things that I mentioned. And It’ll do it to everybody, but it will do it to different degrees. So I would say that virtually everybody, going on a low protein, non fiber carbohydrate diet will be beneficial. It will be more beneficial for some people than it will be for others. But I can’t find any credible argument that non-fiber carbohydrates – carbohydrates that turn to sugar, would actually be good for somebody.
QUESTION: I’m trying to get my patients to get a glucometer. And everyone test their after meal insulin levels. Do you think that would be a good strategy?
RON
Getting someone to test after meal insulin levels would be great. That’s not as available as far as I know. After meal glucose levels you can test, which isn’t as important. I always thought it would be great to have an insulinometer that you could actually check. I’m more interested, not so much in their after meal glucose than what they wake up with and what they go to bed with. My background is really i the treatment of diabetes and heart disease. I have had great success treating cancer, but I haven’t pushed myself as a cancer doctor.
QUESTION: And the work of Dr. Thomas Seyfreid, is Cancer is a metabolic disease is everything he’s writing about in his research as well.
RON
It’s certainly parallel. This is stuff that’s not new, with the exception of mTOR, which I first talked about almost 10 years ago. 20 years ago I started talking about insulin, and about leptin maybe 15 years ago. So this isn’t new. It just hasn’t made its way into mainstream medicine. I’m hoping that I can start planting seeds here and get some lifesaving use out of this knowledge. Maybe some of the mainstream, eventually, will pick it up, even though there’s no drugs that are pushing this right now.
QUESTION: Lee mentioned carbohydrates and Gerson. You’re talking about a high fat diet. Gerson used a rather ow fat diet. Study after study shows that high fruit and vegetable intake has quite a low risk of cancer. Is there an integration between what you’re saying? I’m not talking about carbohydrates from grains now. I’m talking about carbohydrates from fruit, which have carb.
RON
We’re talking about different types of carbs. If you talk about a lot of carbohydrates from fruits and vegetables, a lot of those carbohydrates are going to be fiber. So they go in and out of you. So it’s actually a lower carbohydrate than if you were to eat grains, where 90% turns into sugar really quickly. And in fruit, it doesn’t turn into glucose and it doesn’t turn into insulin as rapidly. It turns into fructose. Fructose then will turn into fat in the liver, which could be good or bad, depending on what else you eat with it. If it was just fructose you ate, I don’t think it’s going to be as bad, because then you’re going to burn that fat. If you eat grains with that fructose, that would be bad because then you can’t burn the fructose and it just stays in the liver and causes fatty liver.
So what we’re also talking about is better or best. The average U-S diet is so bad really, you can close your eyes, throw a dart and say, “change that” and you’ll improve it. It’s not a matter of improving what a person has been eating. I think we have to look at some of the science behind it to not just “improve” the diet. When you’re facing a foe, and adversary like cancer, you really want to give it your best shot. You want to throw the very best diet you’ve got at it. To do that, you need to know the science behind metabolism. And mTOR science is now really clear, that you need to keep MTOR low if you want to have a shot at really affecting cancer. And it’s been known before that that insulin and IgF are two big components of it, too, so we want to keep that low. We know the nutrients that are affecting it. We know the nutrients that raise insulin IgF. That raise mTOR, that raise leptin. It behooves them to keep those low because we don’t need them. And we’ve got a friend in fat, that’s not going to raise any of it. And as Lee was also saying, the type of fat eat, is really important, too, can affect it. It’s a little bit more complex than just eat any fat. But the basic, I want people to understand, it should be a high fat, very moderate, to almost low protein, and a very low, non-fiber carbohydrate diet, I think it’s going to give you the best shot to both prevent and treat cancer that’s already there.
Thanks
***
This recording was produced by Aurora Recording. 828-944-0177. Aurorarecroding.com





6 comments for “Ron Rosedale – Best Answers for Cancer”